~~~ EBOLA NEWS ~~~
BioAcoustic Biology Research Studio investigates public information and research to incorporate every aspect of everything that affects public health and emotional peace of mind. We are a Research/Education site. Finding TRUE KNOWLEDGE is very hard these days. We are committed to supplying you with all that we can find on a given subject, it is then up to you, to use YOUR DISCERNMENT, to truly know the reality we all share. This is a research, education and self help site.
We are all in this together, the more EVERYONE KNOWS, the better off we ALL will be.
BioAcoustic Biology Research Studio investigates public information and research to incorporate every aspect of everything that affects public health and emotional peace of mind. We are a Research/Education site. Finding TRUE KNOWLEDGE is very hard these days. We are committed to supplying you with all that we can find on a given subject, it is then up to you, to use YOUR DISCERNMENT, to truly know the reality we all share. This is a research, education and self help site.
We are all in this together, the more EVERYONE KNOWS, the better off we ALL will be.
Uproar over US troops'
Ebola quarantine in Italy
Published: 29 Oct 2014
"The decision to put a dozen American soldiers returning from Liberia into quarantine for Ebola at their base near Venice rather than in the United States sparked controversy in Italy on Wednesday."
Ebola quarantine in Italy
Published: 29 Oct 2014
"The decision to put a dozen American soldiers returning from Liberia into quarantine for Ebola at their base near Venice rather than in the United States sparked controversy in Italy on Wednesday."
EbolaGate is actually a Bioweapons
False Flag attack strategy,
with many sophisticated alternative scenarios
by Alfred Lambremont Webre
October 5, 2014
False Flag attack strategy,
with many sophisticated alternative scenarios
by Alfred Lambremont Webre
October 5, 2014
VANCOUVER, BC - EbolaGate is actually a Bioweapons False Flag attack strategy, with many sophisticated alternative scenarios, some of which may or may not materialize as in all false flags. The basic premise is to start an Ebola "outbreak" with a bioweapons attack of the Ebola virus in West African countries where local immune systems and health profiles are compromised, there are unsanitary conditions, little public health care, and martial law quarantines for mass infection can easily be imposed (as when towns of 50,000 persons are now being quarantined rather than the infected persons in the towns). Instead of being treated with known Vitamin C and immune system treatments, local populaitons are given ineffective treatments, or worse, treatments that are themselves bioweapons. The scenario here, led by WHO, is to covertly maximize infection rates and vector propagation, shred local health care and public order (nurses are now on strike in one country). This scenario is aimed at (1) creating a base for an African Bioweapons genocide, long sought because of the mineral, oil and gas wealth of Africa [Think of the US Rangers infecting of South Africa with the AIDS virus embedded in the small pox vaccine in the mid 1990s] (2) Providing the jumping-off point for mutation of the EbolaGate viruses and their traveling via air travel, sea travel, land, to Europe, India, Asia, and North and South America. In North America there awaits a sophisticated Ebola Gate False Flag machine led by WHO-CDC [Nazi-CIA] and Martial law regulations signed by George Bush I & II, Clinton, and Obama that can mandate FEMA incarceration and mass vaccinations with EbolaGate vaccines that maim or kill as part of the depopulation plan.
To see the estimated death toll, under current infection rates of Ebola gate by June 2016 of Infected persons: 4,707,573,324 [4.7 Billion] Dead persons: 2,877,739,573 [2.8 billion] please go to:
Regularly Updated! Deadly Ebola Virus Outbreak - EbolaGate
http://exopolitics.blogs.com/ebolagate/2014/09/regularly-updated-deadly-ebola-virus-outbreak-.html
References:
Alfred Webre: Plan A is Martial Law; Plan B is Ebola. Awareness and Critical Mass can deconstruct planned extermination
http://exopolitics.blogs.com/breaking_news/2014/08/alfred-webre-plan-a-is-martial-law-plan-b-is-ebola-awareness-and-critical-mass-can-deconstruct-planned-extermination.html
EbolaGate is actually a Bioweapons False Flag attack strategy, with many sophisticated alternative scenarios
http://exopolitics.blogs.com/ebolagate/2014/09/ebolagate-is-actually-a-bioweapons-false-flag-attack-strategy-with-many-sophisticated-alternative-scenarios.html
To see the estimated death toll, under current infection rates of Ebola gate by June 2016 of Infected persons: 4,707,573,324 [4.7 Billion] Dead persons: 2,877,739,573 [2.8 billion] please go to:
Regularly Updated! Deadly Ebola Virus Outbreak - EbolaGate
http://exopolitics.blogs.com/ebolagate/2014/09/regularly-updated-deadly-ebola-virus-outbreak-.html
References:
Alfred Webre: Plan A is Martial Law; Plan B is Ebola. Awareness and Critical Mass can deconstruct planned extermination
http://exopolitics.blogs.com/breaking_news/2014/08/alfred-webre-plan-a-is-martial-law-plan-b-is-ebola-awareness-and-critical-mass-can-deconstruct-planned-extermination.html
EbolaGate is actually a Bioweapons False Flag attack strategy, with many sophisticated alternative scenarios
http://exopolitics.blogs.com/ebolagate/2014/09/ebolagate-is-actually-a-bioweapons-false-flag-attack-strategy-with-many-sophisticated-alternative-scenarios.html
Do these ten pieces of evidence prove the U.S. government
is actively encouraging
an Ebola outbreak in America?
by Mike Adams, the Health Ranger
October 3, 2014
is actively encouraging
an Ebola outbreak in America?
by Mike Adams, the Health Ranger
October 3, 2014
(NaturalNews) The more closely our team investigates the facts about Ebola here at Natural News, the more I'm convinced the United States government is intentionally trying to increase the spread of the outbreak rather than contain it. I realize this assertion may sound outlandish, but review the evidence below and decide for yourself. This story is extensively sourced with verifiable links.
As microbiologist Dr. Gil Mobley recently said in protest of all the lies and disinformation, "CDC is lying! ... [and] If they're not lying, they are grossly incompetent." [1]
Here are the top ten pieces of evidence that point to the U.S. government seemingly wanting to see Ebola spread even more. Because, just as Dr. Mobley says, if all this isn't intentional, then it's a showcase of extreme incompetence on the part of government:
As microbiologist Dr. Gil Mobley recently said in protest of all the lies and disinformation, "CDC is lying! ... [and] If they're not lying, they are grossly incompetent." [1]
Here are the top ten pieces of evidence that point to the U.S. government seemingly wanting to see Ebola spread even more. Because, just as Dr. Mobley says, if all this isn't intentional, then it's a showcase of extreme incompetence on the part of government:
#1) Obama refuses to halt air travelers from infected countries from entering the United States
#2) Texas family is quarantined in a home that still hasn't been cleaned or decontaminated
READ ALL AT
#2) Texas family is quarantined in a home that still hasn't been cleaned or decontaminated
READ ALL AT
For years some of us have been watching the efforts of the globalists to roll out a pandemic. Parents Against Mandatory Vaccines is just one of many [orgs, groups] tracking this effort and monitoring the CDC and the WHO.
Parents Against Mandatory Vaccines has established a seven step response to the false flag ebola campaign. All are most welcome to review and utilize this information as they see fit. It is important that we educate ourselves so we cannot be manipulated by fear . . . as has been done to us so many times before.
Ebola pandemic response plan
Those in vaccine-aware organizations have stopped pandemic agendas before and if we all take this threat seriously, we can do it again. Hopefully we can also cause irreparable damage to the creditability of the CDC so they can no longer manipulate us, scare us, and threaten the health of ourselves and our children . . . ever again.
SOURCE:http://parentsagainstmandatoryvaccines.wikispaces.com/Seven+Step+Ebola+Response+Plan
SEVEN STEP EBOLA RESPONSE PLAN: Parents Against Mandatory Vaccines - EbolaGate
http://exopolitics.blogs.com/ebolagate/2014/10/seven-step-ebola-response-plan-parents-against-mandatory-vaccines.html
Parents Against Mandatory Vaccines has established a seven step response to the false flag ebola campaign. All are most welcome to review and utilize this information as they see fit. It is important that we educate ourselves so we cannot be manipulated by fear . . . as has been done to us so many times before.
Ebola pandemic response plan
- Recognize that for many reasons, including the establishment of a BRICs economic alliance, the US petrodollar is faltering. The ebola card is most likely being played now as a distraction to that fact and the potential economic carnage this change might cause.
- Know and understand the US is a corporation as is the Center for Disease Control (CDC) and the World Health Organization. As such, they are bound by the law of contracts. [Supreme Court Bond v UNITED STATES]
- Help destroy the credibility of the CDC (long overdue) by reading this page, circulating this link, and handing out this brochure
- Know and understand that a media 'playbook' has been formulated and is now being used to create fear in the general population. Print out these 10 steps so you can watch the psyop and prove to yourself that it is only a psyop. Familiar yourselves with the FACTS as they are being reported at TruthSector.com andNoMoreFakeNews.com
- Do Not Consent to be vaccinated or forced into isolation. Review the info and print out a Pocket Card //Notice of Non-Consent// to carry with you.
- Do what you can to insure your immunity is strong [Vitamin C and sunshine, for example.]
- Don't allow your critical thinking skills to be neutralized by fear. Remember, that is their goal and that is how those that wish to control the planet have successfully manipulated us before . . . many times. Schedule time for joyful experiences and walks in the park.
Those in vaccine-aware organizations have stopped pandemic agendas before and if we all take this threat seriously, we can do it again. Hopefully we can also cause irreparable damage to the creditability of the CDC so they can no longer manipulate us, scare us, and threaten the health of ourselves and our children . . . ever again.
SOURCE:http://parentsagainstmandatoryvaccines.wikispaces.com/Seven+Step+Ebola+Response+Plan
SEVEN STEP EBOLA RESPONSE PLAN: Parents Against Mandatory Vaccines - EbolaGate
http://exopolitics.blogs.com/ebolagate/2014/10/seven-step-ebola-response-plan-parents-against-mandatory-vaccines.html
Addressing Pandemic Threats:
Lack of Forethought or
Man-Made Crisis of
Deliberate Proportions?
Lack of Forethought or
Man-Made Crisis of
Deliberate Proportions?
Small Appalachian research facility is publicly distributing Ebola-Zaire biomarker software in the hope of collecting data to mitigate the pandemic threat using frequency-based Star Trek Proficiency. The results have the potential to guide and identify the threatened pandemic while creating a space-age math- based-medicine resolution to manage wellness.
Albany, Ohio – September 11, 2014 The Institute of BioAcoustic Biology is only one facility that has warned of disastrous pandemic threats resulting from resistant Superbugs combined with no significant strategies to handle such a massive threat.
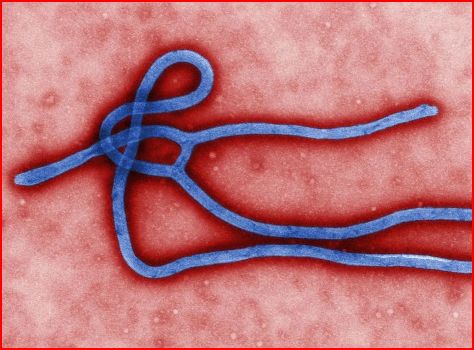
Such a scenario is fast unfolding in Africa; a complete meltdown of the health system as officials attempt to deal with the crisis of Ebola: Zaire. Ebola fever is an infectious and generally fatal disease, discernible by fever and severe internal bleeding; spread through contact with infected body fluids.
Perceived as untreatable, an Ebola infiltration has no known cure; but is that so? Many claim that the “cures” are being withheld by those in authority; others tout nutritional remedies.
Is this wretched governmental response an inadvertent lack of preparation or a man-made crisis of epic proportions designed as a financial bonanza to accomplish a “culling of useless eaters”?
For many years a small research institute in Ohio, USA, the Institute of BioAcoustic Biology & Sound Health, has been researching the use of low frequency sound to influence the eradication of such invaders as Herpes, Epstein Barr, Candida, Chlamydia Pneumonia, colds, flu, sinus and bronchial infections.
Is this wretched response an inadvertent lack of preparation or a man-made crisis of epic proportions designed as a financial bonanza to accomplish a deliberate "culling of useless eaters"?
These studies concluded that each pathogen has a unique set of frequency-based patterns of Genes, Proteins and Activators. For example, a measles Gene is passed from one person to the next. The microbe establishes a colony conjointly with the host, a human body, causing a release of toxins which in turn create an inflammatory response. The lack of Vitamin C might be seen as an Activator for the common cold.
For several years the Institute has publicly released math-based antidotes correlating the information with each flu strain announced by the US Center for Disease Control (CDC.) Each year the frequencies associated with upcoming flu threats seemed to display more sophisticated mathematical properties.
Nature-made pathogens appear to have diffused patterns of unrelated frequencies while man-made pathogens have a more fixed pattern; making them identifiable as synthetic. In the past this lack of consistent patterning allowed for the extrapolation and creation of uncomplicated frequency based antidotes which were tested with encouraging results.
After evaluating these patterns for several consecutive years, recognizable configurations emerge that allowed a comparison of the mathematical formats of man-made prophylactic remedies and vaccinations with the asymmetrical math configurations associated with natural flus. For instance, Gardasil vaccinations clearly show juxtaposed correlations indicating the formulations were likely mathematically conceived.
The present strains of Ebola that are reported to have no cure have been decoded by the BioAcoustic Biology Institute. The bio-frequency extrapolations - that would allow the creation of simple math-based antidotes - were not possible. The seemingly unnatural math permutations thwarted a simple solution. That is not to say that no potential frequency based antidotes are possible; quite the contrary, the approach just needs to be a bit more creative and visionary.
It is obvious, that over the last few years the CDC flu recommendations have “changed” to create a unique situation: The Antidote for one type of flu has become the Activator of a different strain for that same year; making it impossible to use a straightforward computation to create a numeric antidote. If someone is attempting to prevent a frequency-based solution; this would be a perfect scheme.
Extrapolation from previous results provide no absolute proof but based on previous experience the frequency biomarkers decoded for several current strains of Ebola should provide an extraordinary path to provide efficacy.
A more comprehensive understanding of human biology, using frequency as a basis, may quickly move humanity toward space-age resolutions if this modality can be validated on a large scale. Access to a Level IV facility will be necessary to confirm efficacy. If what has been demonstrated with previous pathogens can be integrated using the Ebola biomarkers, this protocol may lay an appropriate foundation to combat for any resistant pathogen, forever.
The Institute of BioAcoustic Biology has agrees to freely distribute these Rife-determined frequency-based antidotes to anyone willing to provide resulting data. As a remedy against these present threats emerge, the potential to remediate any issues using match as medicine may evolve.
Many researchers warned that superbugs were inevitable; a total different avenue to defend against them must be put in place. What is happening to our planet with the surge of Ebola needs to be met with extraordinary measures that do not further jeopardize our health or genetic make-up. At present there is a overall failure of those in authority to take charge of the situation, contain it and keep the populace safe. The answer seems to be beyond the boundaries of conventional science.
The Institute of BioAcoustic Biology has agreed to freely distribute these Rife determined frequency-based antidotes with any country or legitimate agency that has the authority and expertise to test the theories. Additionally as a remedy against these present threats emerge, the potential to remediate any issues using math as medicine may evolve.
For the moment and for legal reasons we have published an abbreviated version of the Gene, Activator and Protein strains that are appropriate for the public. Antidotes are factors that could BioAcoustically remedy the intrusion by any of the strains. Competitors compete with the pathogens for metabolic dominance.
A chart was compiled using the sequencing patterns of the 2014 out-break of Zaire Ebola strains. BioAcoustically Speaking, these frequencies, in combination, primarily seek to optimize Immune, Liver and Kidney issues. We limited the Antidotes and Competitors listings to substances that would be readily available to the public.
Efficacy has not been established using this protocol. WARNING:
Do not use these frequencies if you do not have complete confidence in what you are doing. Absolutely do not use these frequencies unless you have the support of an expert who knows how to appropriately use Rife-Based Frequency Equivalent™(FE) Antidotes.
Available at http://www.soundhealthoptions.com/#!articles/cis
Some of the reasons that allow the proposition that these new strains may be man-made are listed below. Perhaps it is all coincidence!
Human BioAcoustic Biology is a novel field of study pioneered by Sharry Edwards, MEd. Many documentaries verify the protocol; one of the most significant videos titled, Miracles of nonMedicine, is available from www. SoundHealthOptions.com, DOWNLOADS, Secret Stash. Edwards has been declared the originating pioneer of this novel technique by the Duke Encyclopedia of New Medicine. AT&T has declared bioacoustics as the “medicine of the future”.
Out of thousands of possible numeric combinations it seems unlikely that some of these frequency sets used to BioAcousticlly identify Ebola indications would turn-out to be direct mathematically counterbalances to one another. This means that numeric antidotes would defeat each other as possible remedies. Such coincidence is hard to believe!
*Frequency Equivalent™(FE), a term coined by Sharry Edwards, MEd to indicate a numeric representation of a person, place, thing or emotion.
References:
Emergence of Zaire Ebola Virus Disease in Guinea — Preliminary Report
April 16, 2014DOI: 10.1056/NEJMoa1404505.Sylvain Baize, Ph.D., et al
http://www.huffingtonpost.co.uk/2014/08/06/ebola-treatment-funding-vaccine_n_5653826.html
Duke Encyclopedia of New Medicine, 2006, compiled by the Center for Integrative Medicine at Duke University, pp 566.
Courtesy of: Sharry Edwards
Sound Health Options.com
Such a scenario is fast unfolding in Africa; a complete meltdown of the health system as officials attempt to deal with the crisis of Ebola: Zaire. Ebola fever is an infectious and generally fatal disease, discernible by fever and severe internal bleeding; spread through contact with infected body fluids.
Perceived as untreatable, an Ebola infiltration has no known cure; but is that so? Many claim that the “cures” are being withheld by those in authority; others tout nutritional remedies.
Is this wretched governmental response an inadvertent lack of preparation or a man-made crisis of epic proportions designed as a financial bonanza to accomplish a “culling of useless eaters”?
For many years a small research institute in Ohio, USA, the Institute of BioAcoustic Biology & Sound Health, has been researching the use of low frequency sound to influence the eradication of such invaders as Herpes, Epstein Barr, Candida, Chlamydia Pneumonia, colds, flu, sinus and bronchial infections.
Is this wretched response an inadvertent lack of preparation or a man-made crisis of epic proportions designed as a financial bonanza to accomplish a deliberate "culling of useless eaters"?
These studies concluded that each pathogen has a unique set of frequency-based patterns of Genes, Proteins and Activators. For example, a measles Gene is passed from one person to the next. The microbe establishes a colony conjointly with the host, a human body, causing a release of toxins which in turn create an inflammatory response. The lack of Vitamin C might be seen as an Activator for the common cold.
For several years the Institute has publicly released math-based antidotes correlating the information with each flu strain announced by the US Center for Disease Control (CDC.) Each year the frequencies associated with upcoming flu threats seemed to display more sophisticated mathematical properties.
Nature-made pathogens appear to have diffused patterns of unrelated frequencies while man-made pathogens have a more fixed pattern; making them identifiable as synthetic. In the past this lack of consistent patterning allowed for the extrapolation and creation of uncomplicated frequency based antidotes which were tested with encouraging results.
After evaluating these patterns for several consecutive years, recognizable configurations emerge that allowed a comparison of the mathematical formats of man-made prophylactic remedies and vaccinations with the asymmetrical math configurations associated with natural flus. For instance, Gardasil vaccinations clearly show juxtaposed correlations indicating the formulations were likely mathematically conceived.
The present strains of Ebola that are reported to have no cure have been decoded by the BioAcoustic Biology Institute. The bio-frequency extrapolations - that would allow the creation of simple math-based antidotes - were not possible. The seemingly unnatural math permutations thwarted a simple solution. That is not to say that no potential frequency based antidotes are possible; quite the contrary, the approach just needs to be a bit more creative and visionary.
It is obvious, that over the last few years the CDC flu recommendations have “changed” to create a unique situation: The Antidote for one type of flu has become the Activator of a different strain for that same year; making it impossible to use a straightforward computation to create a numeric antidote. If someone is attempting to prevent a frequency-based solution; this would be a perfect scheme.
Extrapolation from previous results provide no absolute proof but based on previous experience the frequency biomarkers decoded for several current strains of Ebola should provide an extraordinary path to provide efficacy.
A more comprehensive understanding of human biology, using frequency as a basis, may quickly move humanity toward space-age resolutions if this modality can be validated on a large scale. Access to a Level IV facility will be necessary to confirm efficacy. If what has been demonstrated with previous pathogens can be integrated using the Ebola biomarkers, this protocol may lay an appropriate foundation to combat for any resistant pathogen, forever.
The Institute of BioAcoustic Biology has agrees to freely distribute these Rife-determined frequency-based antidotes to anyone willing to provide resulting data. As a remedy against these present threats emerge, the potential to remediate any issues using match as medicine may evolve.
Many researchers warned that superbugs were inevitable; a total different avenue to defend against them must be put in place. What is happening to our planet with the surge of Ebola needs to be met with extraordinary measures that do not further jeopardize our health or genetic make-up. At present there is a overall failure of those in authority to take charge of the situation, contain it and keep the populace safe. The answer seems to be beyond the boundaries of conventional science.
The Institute of BioAcoustic Biology has agreed to freely distribute these Rife determined frequency-based antidotes with any country or legitimate agency that has the authority and expertise to test the theories. Additionally as a remedy against these present threats emerge, the potential to remediate any issues using math as medicine may evolve.
For the moment and for legal reasons we have published an abbreviated version of the Gene, Activator and Protein strains that are appropriate for the public. Antidotes are factors that could BioAcoustically remedy the intrusion by any of the strains. Competitors compete with the pathogens for metabolic dominance.
A chart was compiled using the sequencing patterns of the 2014 out-break of Zaire Ebola strains. BioAcoustically Speaking, these frequencies, in combination, primarily seek to optimize Immune, Liver and Kidney issues. We limited the Antidotes and Competitors listings to substances that would be readily available to the public.
Efficacy has not been established using this protocol. WARNING:
Do not use these frequencies if you do not have complete confidence in what you are doing. Absolutely do not use these frequencies unless you have the support of an expert who knows how to appropriately use Rife-Based Frequency Equivalent™(FE) Antidotes.
Available at http://www.soundhealthoptions.com/#!articles/cis
Some of the reasons that allow the proposition that these new strains may be man-made are listed below. Perhaps it is all coincidence!
- One of the Ebola Strain Proteins is the same FE* as a Hemophiliac Gene (Hemophilia is a bleeding disorder which acts similarly to Ebola symptoms).
- Fibrin (involved in blood clotting) is the same FE* as the competitor of the Strain 47 Protein.
- Fibrinogen (helps support blood clotting) is the same Frequency Equivalent™ of the Antidote frequency for strain 48.
- The FE™ Antidote of Ebola Strain 49 is the Activator of the Ebola Gene frequency, indicating that providing a frequency-based antidote of strain 49 may activate the Ebola Gene itself.
Human BioAcoustic Biology is a novel field of study pioneered by Sharry Edwards, MEd. Many documentaries verify the protocol; one of the most significant videos titled, Miracles of nonMedicine, is available from www. SoundHealthOptions.com, DOWNLOADS, Secret Stash. Edwards has been declared the originating pioneer of this novel technique by the Duke Encyclopedia of New Medicine. AT&T has declared bioacoustics as the “medicine of the future”.
Out of thousands of possible numeric combinations it seems unlikely that some of these frequency sets used to BioAcousticlly identify Ebola indications would turn-out to be direct mathematically counterbalances to one another. This means that numeric antidotes would defeat each other as possible remedies. Such coincidence is hard to believe!
*Frequency Equivalent™(FE), a term coined by Sharry Edwards, MEd to indicate a numeric representation of a person, place, thing or emotion.
References:
Emergence of Zaire Ebola Virus Disease in Guinea — Preliminary Report
April 16, 2014DOI: 10.1056/NEJMoa1404505.Sylvain Baize, Ph.D., et al
http://www.huffingtonpost.co.uk/2014/08/06/ebola-treatment-funding-vaccine_n_5653826.html
Duke Encyclopedia of New Medicine, 2006, compiled by the Center for Integrative Medicine at Duke University, pp 566.
Courtesy of: Sharry Edwards
Sound Health Options.com
LIBERIA'S LARGEST NEWSPAPER:
US DEPT. OF DEFENSE
'MANUFACTURED' EBOLA, AIDS
by FRANCES MARTEL
10 Sep 2014
US DEPT. OF DEFENSE
'MANUFACTURED' EBOLA, AIDS
by FRANCES MARTEL
10 Sep 2014
The largest newspaper in Monrovia, Liberia, has published an outrageous conspiracy theory column arguing that the United States is directly responsible for scientifically engineering the Ebola virus in a bioterrorism lab and injecting Africans with it through the guise of vaccinations.The wildly accusatory article, by Dr. Cyril Broderick, a former professor of Plant Pathology at the University of Liberia’s College of Agriculture and Forestry, claims the Ebola virus--and HIV--are products of the Cold War. Titled "Ebola, AIDS Manufactured By Western Pharmaceuticals, US DoD?" Broderick's article claims--using evidence such as the science fiction novel The Hot Zone--that the Department of Defense unwittingly used Africans to test experimental bioweapons by pretending they were vaccinating them against disease. "Reports," he argues, without actually citing any reports, "narrate stories of the US Department of Defense (DoD) funding Ebola trials on humans, trials which started just weeks before the Ebola outbreak in Guinea and Sierra Leone."
He cites the 1996 Leonard Horowitz work Emerging Viruses: AIDS And Ebola: Nature, Accident or Intentional? to claim that a facility in Maryland had "a lot of problems with strange illnesses" during the Cold War, a clear sign that many of these diseases were the product of U.S. experimentation to Broderick. He also claims the book definitively proves "the existence of an American Military-Medical-Industry that conducts biological weapons tests under the guise of administering vaccinations to control diseases and improve the health of 'black Africans overseas.'”
Broderick also accuses the World Health Organization (WHO) and Doctors Without Borders of bringing Ebola to Africa through vaccination programs. He asserts, too, that "many reports also conclude that the US government has a viral fever bioterrorism research laboratory in Kenema, a town at the epicentre of the Ebola outbreak in West Africa."
Perhaps most outrageously, Broderick attempts to cite a real source, The Guardian, alleging that a report in the paper said, "The US government funding of Ebola trials on healthy humans comes amid warnings by top scientists in Harvard and Yale that such virus experiments risk triggering a worldwide pandemic." A routine Internet search finds no evidence that such a sentence was ever written in the pages of The Guardian.
Broderick concludes, somehow, by calling for a class action lawsuit against Tulane University to combat the Ebola virus. "Africa must not relegate the Continent to become the locality for disposal and the deposition of hazardous chemicals, dangerous drugs, and chemical or biological agents of emerging diseases," he rails.
The text, for Westerners, is undoubtedly outrageous and easily dismissible. It is not the first time for such rumors in Africa, however; the last time, it was discovered that the KGB had planted stories in African media, accusing the United States of inventing the AIDS virus. But for Africans, many of whom operate under assumptions that they are under the constant threat of Western exploitation due to a history of colonialism, such a report is not so easy to ignore. As experts have noted, much of the violent resistance to Western science that has led to such a rapid spread of the virus is the product of a rejection of what Africans perceive as Western "paternalism" in coming to their continent and offering medical care.
That the Liberian Daily Observer is currently featuring it on its front page is of particular concern. The Observer is Liberia's largest newspaper, with a circulation of 30,000, mostly in the capital, Monrovia. Given the backdrop of panic into which this "report" is being disseminated, the consequences could be devastating for Liberia. The nation is already fending off significant distrust from the Liberian people--the kind of distrust that makes family members kidnap their own relatives out of hospitals to bring them to traditional herbalists for treatment they trust, the kind of distrust that triggers mob attacks on medical facilities run by the WHO and Doctors Without Borders and looting of healthcare buildings.
Running such a column in a climate of extreme distrust is, to say the least, unfathomably irresponsible on the part of the Observer. With such resistance from Africa's communities to finding a cure, the Ebola virus will only continue to spread, and having claimed more than 2,000 lives already, Ebola can only grow as an existential threat to West African governments.
He cites the 1996 Leonard Horowitz work Emerging Viruses: AIDS And Ebola: Nature, Accident or Intentional? to claim that a facility in Maryland had "a lot of problems with strange illnesses" during the Cold War, a clear sign that many of these diseases were the product of U.S. experimentation to Broderick. He also claims the book definitively proves "the existence of an American Military-Medical-Industry that conducts biological weapons tests under the guise of administering vaccinations to control diseases and improve the health of 'black Africans overseas.'”
Broderick also accuses the World Health Organization (WHO) and Doctors Without Borders of bringing Ebola to Africa through vaccination programs. He asserts, too, that "many reports also conclude that the US government has a viral fever bioterrorism research laboratory in Kenema, a town at the epicentre of the Ebola outbreak in West Africa."
Perhaps most outrageously, Broderick attempts to cite a real source, The Guardian, alleging that a report in the paper said, "The US government funding of Ebola trials on healthy humans comes amid warnings by top scientists in Harvard and Yale that such virus experiments risk triggering a worldwide pandemic." A routine Internet search finds no evidence that such a sentence was ever written in the pages of The Guardian.
Broderick concludes, somehow, by calling for a class action lawsuit against Tulane University to combat the Ebola virus. "Africa must not relegate the Continent to become the locality for disposal and the deposition of hazardous chemicals, dangerous drugs, and chemical or biological agents of emerging diseases," he rails.
The text, for Westerners, is undoubtedly outrageous and easily dismissible. It is not the first time for such rumors in Africa, however; the last time, it was discovered that the KGB had planted stories in African media, accusing the United States of inventing the AIDS virus. But for Africans, many of whom operate under assumptions that they are under the constant threat of Western exploitation due to a history of colonialism, such a report is not so easy to ignore. As experts have noted, much of the violent resistance to Western science that has led to such a rapid spread of the virus is the product of a rejection of what Africans perceive as Western "paternalism" in coming to their continent and offering medical care.
That the Liberian Daily Observer is currently featuring it on its front page is of particular concern. The Observer is Liberia's largest newspaper, with a circulation of 30,000, mostly in the capital, Monrovia. Given the backdrop of panic into which this "report" is being disseminated, the consequences could be devastating for Liberia. The nation is already fending off significant distrust from the Liberian people--the kind of distrust that makes family members kidnap their own relatives out of hospitals to bring them to traditional herbalists for treatment they trust, the kind of distrust that triggers mob attacks on medical facilities run by the WHO and Doctors Without Borders and looting of healthcare buildings.
Running such a column in a climate of extreme distrust is, to say the least, unfathomably irresponsible on the part of the Observer. With such resistance from Africa's communities to finding a cure, the Ebola virus will only continue to spread, and having claimed more than 2,000 lives already, Ebola can only grow as an existential threat to West African governments.
HHS READIES U.S. HOSPITALS FOR EBOLA
States kept in the dark about severity of the often fatal disease
by KURT NIMMO | INFOWARS.COM SEPTEMBER 17, 2014
Oklahoma Republican State Rep. Mike Ritze told a local television station the Department of Health and Human Services is examining the readiness of hospitals in the state for an influx of Ebola patients.
According to the former chairman of the Tulsa County Republican Party, the HHS is also checking hospitals in New Mexico and other states.
The Oklahoma State Department of Health believes all 50 states have received inquiries from the federal agency about the readiness to accept Ebola patients, according to KFOR in Oklahoma City.
“This may just be a routine inquiry, but it strikes me as curious given the recent outbreak of Ebola cases in West Africa,” said Ritze. “At this point, there is no need to panic, but it would be helpful to get some accurate information from our state and federal health organizations so we know how severe the threat may be.”
The Center for Disease Control and Prevention has also told hospitals to prepare for an outbreak in the United States. The CDC released a revised checklist on Ebola preparedness for all hospitals on Monday.
“It’s gone beyond an Ebola crisis to a humanitarian crisis,” said Dr. Steve Monroe of the CDC. “It does require more of a U.S. government-wide response, more than just CDC.”
On Tuesday Obama visited the CDC headquarters in Atlanta and met with staff there.
“This is a daunting task, but here’s what gives us hope. The world knows how to fight this disease. It’s not a mystery. We know the science. We know how to prevent it from spreading. We know how to care for those who contract it. We know that if we take the proper steps, we can save lives. But we have to act fast,” Obama said.
Obama characterized the African outbreak as a threat to global security. “The reality is that this epidemic is going to get worse before it gets better,” he predicted.
Obama announced a plan to send 3,000 U.S. troops, including engineers and medical personnel, to Monrovia, the capital of Liberia, where a regional command center will be established and commanded by Major General Darryl Williams.
Doctors Without Borders and other NGOs are wary of military involvement in the growing health crisis.
“In this particular case, the Ebola emergency is so severe and the logistical challenges are so serious and seem so insurmountable that you have humanitarian actors that are normally very resistant to any kind of military aid asking for the military to get involved,” said Laura Seay, a Colby College assistant professor of government specializing in African issues.
“This is one of those things where you have to be careful what you wish for,” Seay said.
According to the former chairman of the Tulsa County Republican Party, the HHS is also checking hospitals in New Mexico and other states.
The Oklahoma State Department of Health believes all 50 states have received inquiries from the federal agency about the readiness to accept Ebola patients, according to KFOR in Oklahoma City.
“This may just be a routine inquiry, but it strikes me as curious given the recent outbreak of Ebola cases in West Africa,” said Ritze. “At this point, there is no need to panic, but it would be helpful to get some accurate information from our state and federal health organizations so we know how severe the threat may be.”
The Center for Disease Control and Prevention has also told hospitals to prepare for an outbreak in the United States. The CDC released a revised checklist on Ebola preparedness for all hospitals on Monday.
“It’s gone beyond an Ebola crisis to a humanitarian crisis,” said Dr. Steve Monroe of the CDC. “It does require more of a U.S. government-wide response, more than just CDC.”
On Tuesday Obama visited the CDC headquarters in Atlanta and met with staff there.
“This is a daunting task, but here’s what gives us hope. The world knows how to fight this disease. It’s not a mystery. We know the science. We know how to prevent it from spreading. We know how to care for those who contract it. We know that if we take the proper steps, we can save lives. But we have to act fast,” Obama said.
Obama characterized the African outbreak as a threat to global security. “The reality is that this epidemic is going to get worse before it gets better,” he predicted.
Obama announced a plan to send 3,000 U.S. troops, including engineers and medical personnel, to Monrovia, the capital of Liberia, where a regional command center will be established and commanded by Major General Darryl Williams.
Doctors Without Borders and other NGOs are wary of military involvement in the growing health crisis.
“In this particular case, the Ebola emergency is so severe and the logistical challenges are so serious and seem so insurmountable that you have humanitarian actors that are normally very resistant to any kind of military aid asking for the military to get involved,” said Laura Seay, a Colby College assistant professor of government specializing in African issues.
“This is one of those things where you have to be careful what you wish for,” Seay said.

Image Credits: Sebástian Freire / Flickr (Medical workers)
COMPUTER MODELS TELL US THAT THIS
EBOLA PANDEMIC COULD SOON KILL MILLIONS
We could potentially be on the verge of
the greatest health crisis that any of us have ever seen
EBOLA PANDEMIC COULD SOON KILL MILLIONS
We could potentially be on the verge of
the greatest health crisis that any of us have ever seen
by MICHAEL SNYDER | ECONOMIC COLLAPSE SEPTEMBER 16, 2014
We could potentially be on the verge of the greatest health crisis that any of us have ever seen. The number of Ebola cases in Africa has approximately doubled over the past three weeks, and scientific computer models tell us that this Ebola pandemic could ultimately end up killing millions of us – especially if it starts spreading on other continents. At first, many assumed that this Ebola outbreak would be just like all the others – that it would flare up for a little while and then it would completely fade away. But that has not happened this time. Instead, this epidemic has seemed to pick up momentum with each passing week. Despite extraordinary precautions, hundreds of health workers have gotten the virus, and the head of the CDC says that the spread of Ebola is “spiraling out of control” and that it is “going to get worse in the very near future.” For those that have thought that all of this talk about Ebola was just “fearmongering”, it is time for you to wake up.
Right now, the World Health Organization says that we could see the total number of Ebola cases reach 20,000 nine months from now. But computer models created for the National Institutes of Health and the Department of Defense are projecting that Ebola could soon be growing at a rate of 20,000 cases per month…
The Ebola epidemic affecting West Africa is predicted to last a further 12 to 18 months, according to U.S. scientists.
Epidemiologists have been creating computer models of the Ebola epidemic for the National Institutes of Health and the Defense Department.
The model they have created is a far less optimistic estimate than that of the World Health Organization (WHO), which last month said it hoped to contain the outbreak within nine months and 20,000 total cases.
The New York Times reports that various researchers have said the virus could grow at a rate that could be closer to 20,000 per month.
The WHO is sticking to its estimates, a spokesman said Friday.
Other scientists are even more pessimistic.
For example, a model created jointly by a researcher at the University of Tokyo and a researcher at Arizona State University has produced a “worst-case scenario” of 277,124 Ebola cases by the end of this year…
The Eurosurveillance paper, by two researchers from the University of Tokyo and Arizona State University, attempts to derive what the reproductive rate has been in Guinea, Liberia and Sierra Leone. (Note for actual epidemiology geeks: The calculation is for the effective reproductive number, pegged to a point in time, hence actually Rt.) They come up with an R of at least 1, and in some cases 2; that is, at certain points, sick persons have caused disease in two others.
You can see how that could quickly get out of hand, and in fact, that is what the researchers predict. Here is their stop-you-in-your-tracks assessment:
In a worst-case hypothetical scenario, should the outbreak continue with recent trends, the case burden could gain an additional 77,181 to 277,124 casesby the end of 2014.
That is a jaw-dropping number.
If we do see an explosion like that, how many millions of cases will we see by the time 2015 is through?
A different model has produced an even more jaw-dropping number.
An “econometric simulation model” created by Francis Smart at Michigan State University is predicting that a whopping 1.2 million people will die from Ebola in the next six months…
An econometric simulation model based on the assumption the World Health Organization and others will be unable to control the Ebola outbreak in West Africa predicts 1.2 million people will die from the disease in the next six months.
Six months is the minimum time the WHO projects will be necessary to contain the epidemic.
In his analysis, econometrics research assistantFrancis Smart at Michigan State University took seriously the conclusions of Canadian researchers who proved the strain of Ebola in the current West African epidemic could go airborne.
The Ebola virus could be transmitted between humans through breathing, Smart says.
In developing the model, Smart began with WHO’s Aug. 28 statement that the Ebola epidemic in West Africa could afflict more than 20,000 people before it is brought under control.
That has got to be the worst possible number, right? Wrong.
The other day a prominent German virologist came forward and declared that “it is too late” to stop Ebola and that five million people will die in Sierra Leone and Liberia alone…
A top German virologist has caused shockwaves by asserting that it’s too late to halt the spread of Ebola in Sierra Leone and Liberia and that five million people will die, noting that efforts should now be focused on stopping the transmission of the virus to other countries.
Jonas Schmidt-Chanasit of the Bernhard Nocht Institute for Tropical Medicine in Hamburg told Germany’s Deutsche Welle that hope is all but lost for the inhabitants of Sierra Leone and Liberia and that the virus will only “burn itself out” when it has infected the entire population and killed five million people.
“The right time to get this epidemic under control in these countries has been missed,” said Schmidt-Chanasit. “That time was May and June. “Now it is too late.”
So which of the numbers discussed above are accurate? Only time will tell.
Meanwhile, the U.S. federal government is feverishly preparing for the worst.
This week we learned that Barack Obama is going to ask Congress for 88 million dollars for the purpose of conducting “a major Ebola offensive” in Africa.
Granted, Obama will ask Congress for money at the drop of a hat these days. He wants 500 million dollars to arm the allies of ISIS and his reckless spending has been one of the primary factors why the U.S. national debt has risen by more than a trillion dollars over the past 12 months.
But it is still noteworthy.
Even more noteworthy is the fact that the U.S. State Department has just ordered 160,000 Hazmat suits…
The U.S. State Department has ordered 160,000 Hazmat suits for Ebola, prompting concerns that the federal government is anticipating the rapid spread of a virus that has already claimed an unprecedented number of lives.
In a press release posted by Market Watch, Lakeland Industries, a manufacturer of industrial protective clothing for first responders, announced that it had signaled its intention “to join the fight against the spread of Ebola” by encouraging other suppliers to meet the huge demand created by the U.S. State Department’s order of 160,000 hazmat suits.
“With the U.S. State Department alone putting out a bid for 160,000 suits, we encourage all protective apparel companies to increase their manufacturing capacity for sealed seam garments so that our industry can do its part in addressing this threat to global health,” states the press release.
The huge bulk order of hazmat suits for Ebola has stoked concerns that the U.S. government expects the virus to continue to ravage countries in west Africa and may also be concerned about an outbreak inside the United States.
You don’t order that many Hazmat suits unless you are anticipating an outbreak of apocalyptic proportions.
And the CDC has just issued a six page Ebola checklist to hospitals to help them spot potential Ebola patients in America…
The Centers for Disease Control and Prevention, warning hospitals and doctors that “now is the time to prepare,” has issued a six-page Ebola “checklist” to help healthcare workers quickly determine if patients are infected.
While the CDC does not believe that there are new cases of Ebola in the United States, the assumption in the checklist is that it is only a matter of time before the virus hits home.
Let us hope and pray that these precautions do not become necessary.
Because if Ebola starts spreading like wildfire in this country, we are going to see pain and suffering beyond anything that most of us have ever imagined.
Just consider what a health worker on the front lines is seeing on a day to day basis…
I wake up each morning – if I have managed to sleep – wondering if this is really happening, or if it is a horror movie. In decades of humanitarian work I have never witnessed such relentless suffering of fellow human beings or felt so completely paralysed and utterly overwhelmed at our inability to provide anything but the most basic, and sometimes less than adequate, care.
I am supervising the suspect tent, which has room for 25 patients who are likely to have Ebola – 80-90% of those we test have the virus. We administer treatment for malaria, start patients on antibiotics, paracetamol, multivitamins, rehydration supplements, food, water and juice while they wait for their results. Sometimes people have arrived too late and die shortly after arriving.
In one afternoon last week I watched five seemingly fit, healthy, young men die. I gave the first a bottle of oral rehydration solution and came back with another for the second. In the half a minute or so in which I had been away the first man died, his bottle of water spilt across the floor. The four others followed in quick succession.
Ebola is truly a terrible, terrible disease.
The moment that cases start popping up in the United States, all of our lives will instantly change.
I hope that you are getting prepared for that.
We could potentially be on the verge of the greatest health crisis that any of us have ever seen. The number of Ebola cases in Africa has approximately doubled over the past three weeks, and scientific computer models tell us that this Ebola pandemic could ultimately end up killing millions of us – especially if it starts spreading on other continents. At first, many assumed that this Ebola outbreak would be just like all the others – that it would flare up for a little while and then it would completely fade away. But that has not happened this time. Instead, this epidemic has seemed to pick up momentum with each passing week. Despite extraordinary precautions, hundreds of health workers have gotten the virus, and the head of the CDC says that the spread of Ebola is “spiraling out of control” and that it is “going to get worse in the very near future.” For those that have thought that all of this talk about Ebola was just “fearmongering”, it is time for you to wake up.
Right now, the World Health Organization says that we could see the total number of Ebola cases reach 20,000 nine months from now. But computer models created for the National Institutes of Health and the Department of Defense are projecting that Ebola could soon be growing at a rate of 20,000 cases per month…
The Ebola epidemic affecting West Africa is predicted to last a further 12 to 18 months, according to U.S. scientists.
Epidemiologists have been creating computer models of the Ebola epidemic for the National Institutes of Health and the Defense Department.
The model they have created is a far less optimistic estimate than that of the World Health Organization (WHO), which last month said it hoped to contain the outbreak within nine months and 20,000 total cases.
The New York Times reports that various researchers have said the virus could grow at a rate that could be closer to 20,000 per month.
The WHO is sticking to its estimates, a spokesman said Friday.
Other scientists are even more pessimistic.
For example, a model created jointly by a researcher at the University of Tokyo and a researcher at Arizona State University has produced a “worst-case scenario” of 277,124 Ebola cases by the end of this year…
The Eurosurveillance paper, by two researchers from the University of Tokyo and Arizona State University, attempts to derive what the reproductive rate has been in Guinea, Liberia and Sierra Leone. (Note for actual epidemiology geeks: The calculation is for the effective reproductive number, pegged to a point in time, hence actually Rt.) They come up with an R of at least 1, and in some cases 2; that is, at certain points, sick persons have caused disease in two others.
You can see how that could quickly get out of hand, and in fact, that is what the researchers predict. Here is their stop-you-in-your-tracks assessment:
In a worst-case hypothetical scenario, should the outbreak continue with recent trends, the case burden could gain an additional 77,181 to 277,124 casesby the end of 2014.
That is a jaw-dropping number.
If we do see an explosion like that, how many millions of cases will we see by the time 2015 is through?
A different model has produced an even more jaw-dropping number.
An “econometric simulation model” created by Francis Smart at Michigan State University is predicting that a whopping 1.2 million people will die from Ebola in the next six months…
An econometric simulation model based on the assumption the World Health Organization and others will be unable to control the Ebola outbreak in West Africa predicts 1.2 million people will die from the disease in the next six months.
Six months is the minimum time the WHO projects will be necessary to contain the epidemic.
In his analysis, econometrics research assistantFrancis Smart at Michigan State University took seriously the conclusions of Canadian researchers who proved the strain of Ebola in the current West African epidemic could go airborne.
The Ebola virus could be transmitted between humans through breathing, Smart says.
In developing the model, Smart began with WHO’s Aug. 28 statement that the Ebola epidemic in West Africa could afflict more than 20,000 people before it is brought under control.
That has got to be the worst possible number, right? Wrong.
The other day a prominent German virologist came forward and declared that “it is too late” to stop Ebola and that five million people will die in Sierra Leone and Liberia alone…
A top German virologist has caused shockwaves by asserting that it’s too late to halt the spread of Ebola in Sierra Leone and Liberia and that five million people will die, noting that efforts should now be focused on stopping the transmission of the virus to other countries.
Jonas Schmidt-Chanasit of the Bernhard Nocht Institute for Tropical Medicine in Hamburg told Germany’s Deutsche Welle that hope is all but lost for the inhabitants of Sierra Leone and Liberia and that the virus will only “burn itself out” when it has infected the entire population and killed five million people.
“The right time to get this epidemic under control in these countries has been missed,” said Schmidt-Chanasit. “That time was May and June. “Now it is too late.”
So which of the numbers discussed above are accurate? Only time will tell.
Meanwhile, the U.S. federal government is feverishly preparing for the worst.
This week we learned that Barack Obama is going to ask Congress for 88 million dollars for the purpose of conducting “a major Ebola offensive” in Africa.
Granted, Obama will ask Congress for money at the drop of a hat these days. He wants 500 million dollars to arm the allies of ISIS and his reckless spending has been one of the primary factors why the U.S. national debt has risen by more than a trillion dollars over the past 12 months.
But it is still noteworthy.
Even more noteworthy is the fact that the U.S. State Department has just ordered 160,000 Hazmat suits…
The U.S. State Department has ordered 160,000 Hazmat suits for Ebola, prompting concerns that the federal government is anticipating the rapid spread of a virus that has already claimed an unprecedented number of lives.
In a press release posted by Market Watch, Lakeland Industries, a manufacturer of industrial protective clothing for first responders, announced that it had signaled its intention “to join the fight against the spread of Ebola” by encouraging other suppliers to meet the huge demand created by the U.S. State Department’s order of 160,000 hazmat suits.
“With the U.S. State Department alone putting out a bid for 160,000 suits, we encourage all protective apparel companies to increase their manufacturing capacity for sealed seam garments so that our industry can do its part in addressing this threat to global health,” states the press release.
The huge bulk order of hazmat suits for Ebola has stoked concerns that the U.S. government expects the virus to continue to ravage countries in west Africa and may also be concerned about an outbreak inside the United States.
You don’t order that many Hazmat suits unless you are anticipating an outbreak of apocalyptic proportions.
And the CDC has just issued a six page Ebola checklist to hospitals to help them spot potential Ebola patients in America…
The Centers for Disease Control and Prevention, warning hospitals and doctors that “now is the time to prepare,” has issued a six-page Ebola “checklist” to help healthcare workers quickly determine if patients are infected.
While the CDC does not believe that there are new cases of Ebola in the United States, the assumption in the checklist is that it is only a matter of time before the virus hits home.
Let us hope and pray that these precautions do not become necessary.
Because if Ebola starts spreading like wildfire in this country, we are going to see pain and suffering beyond anything that most of us have ever imagined.
Just consider what a health worker on the front lines is seeing on a day to day basis…
I wake up each morning – if I have managed to sleep – wondering if this is really happening, or if it is a horror movie. In decades of humanitarian work I have never witnessed such relentless suffering of fellow human beings or felt so completely paralysed and utterly overwhelmed at our inability to provide anything but the most basic, and sometimes less than adequate, care.
I am supervising the suspect tent, which has room for 25 patients who are likely to have Ebola – 80-90% of those we test have the virus. We administer treatment for malaria, start patients on antibiotics, paracetamol, multivitamins, rehydration supplements, food, water and juice while they wait for their results. Sometimes people have arrived too late and die shortly after arriving.
In one afternoon last week I watched five seemingly fit, healthy, young men die. I gave the first a bottle of oral rehydration solution and came back with another for the second. In the half a minute or so in which I had been away the first man died, his bottle of water spilt across the floor. The four others followed in quick succession.
Ebola is truly a terrible, terrible disease.
The moment that cases start popping up in the United States, all of our lives will instantly change.
I hope that you are getting prepared for that.

Image Credits: ganatlguard, Flickr
U.S. STATE DEPARTMENT ORDERS
160,000 EBOLA HAZMAT SUITS
Bulk purchase prompts concerns about spread of deadly epidemic
160,000 EBOLA HAZMAT SUITS
Bulk purchase prompts concerns about spread of deadly epidemic
by PAUL JOSEPH WATSON SEPTEMBER 15, 2014
The U.S. State Department has ordered 160,000 Hazmat suits for Ebola, prompting concerns that the federal government is anticipating the rapid spread of a virus that has already claimed an unprecedented number of lives.
In a press release posted by Market Watch, Lakeland Industries, a manufacturer of industrial protective clothing for first responders, announced that it had signaled its intention “to join the fight against the spread of Ebola” by encouraging other suppliers to meet the huge demand created by the U.S. State Department’s order of 160,000 hazmat suits.
“With the U.S. State Department alone putting out a bid for 160,000 suits, we encourage all protective apparel companies to increase their manufacturing capacity for sealed seam garments so that our industry can do its part in addressing this threat to global health,” states the press release.
The huge bulk order of hazmat suits for Ebola has stoked concerns that the U.S. government expects the virus to continue to ravage countries in west Africa and may also be concerned about an outbreak inside the United States.
Although the State Department has announced that it is planning a “surge” of emergency medical personnel into western Africa, only 1400 federal workers are currently in the region, suggesting that the 160,000 figure is far higher than what would be required merely for sending medical workers abroad.
In a related story, sources from within the Department of Defense have questioned why the Obama administration is implementing a military response to the Ebola epidemic when USAID and the Centers for Disease Control and Prevention are already involved in relief efforts.
“We don’t need to be taking planners away from the CT [counterterrorism] mission, and that is what is going on,” the Defense Department source told Fox News.
As we reported last week, top German virologist Jonas Schmidt-Chanasit caused consternation when he suggested that the battle against Ebola in Sierra Leone and Liberia was lost and that the virus would eventually kill 5 million people.
Evidence that the virus has mutated has led to fears that Ebola could have gone airborne to at least a limited extent.
In an op-ed for the New York Times, Michael T. Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, notes that, “there has been more human-to-human transmission in the past four months than most likely occurred in the last 500 to 1,000 years.”
Osterholm says the premise that Ebola could mutate to become transmissible through the air is a possibility “that virologists are loath to discuss openly but are definitely considering in private.”
Facebook @ https://www.facebook.com/paul.j.watson.71
FOLLOW Paul Joseph Watson @ https://twitter.com/PrisonPlanet
The U.S. State Department has ordered 160,000 Hazmat suits for Ebola, prompting concerns that the federal government is anticipating the rapid spread of a virus that has already claimed an unprecedented number of lives.
In a press release posted by Market Watch, Lakeland Industries, a manufacturer of industrial protective clothing for first responders, announced that it had signaled its intention “to join the fight against the spread of Ebola” by encouraging other suppliers to meet the huge demand created by the U.S. State Department’s order of 160,000 hazmat suits.
“With the U.S. State Department alone putting out a bid for 160,000 suits, we encourage all protective apparel companies to increase their manufacturing capacity for sealed seam garments so that our industry can do its part in addressing this threat to global health,” states the press release.
The huge bulk order of hazmat suits for Ebola has stoked concerns that the U.S. government expects the virus to continue to ravage countries in west Africa and may also be concerned about an outbreak inside the United States.
Although the State Department has announced that it is planning a “surge” of emergency medical personnel into western Africa, only 1400 federal workers are currently in the region, suggesting that the 160,000 figure is far higher than what would be required merely for sending medical workers abroad.
In a related story, sources from within the Department of Defense have questioned why the Obama administration is implementing a military response to the Ebola epidemic when USAID and the Centers for Disease Control and Prevention are already involved in relief efforts.
“We don’t need to be taking planners away from the CT [counterterrorism] mission, and that is what is going on,” the Defense Department source told Fox News.
As we reported last week, top German virologist Jonas Schmidt-Chanasit caused consternation when he suggested that the battle against Ebola in Sierra Leone and Liberia was lost and that the virus would eventually kill 5 million people.
Evidence that the virus has mutated has led to fears that Ebola could have gone airborne to at least a limited extent.
In an op-ed for the New York Times, Michael T. Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota, notes that, “there has been more human-to-human transmission in the past four months than most likely occurred in the last 500 to 1,000 years.”
Osterholm says the premise that Ebola could mutate to become transmissible through the air is a possibility “that virologists are loath to discuss openly but are definitely considering in private.”
Facebook @ https://www.facebook.com/paul.j.watson.71
FOLLOW Paul Joseph Watson @ https://twitter.com/PrisonPlanet

Image Credits: Alex / Flickr
FLASHBACK: EBOLA GOES AIRBORNE,
CAUSES OUTBREAK IN MEDICAL LAB
Ebola mutated into an airborne virus back in 1989
CAUSES OUTBREAK IN MEDICAL LAB
Ebola mutated into an airborne virus back in 1989
by KIT DANIELS | INFOWARS.COM SEPTEMBER 15, 2014
A mutated Ebola virus likely spread through the ventilation system of a Virginia medical lab in 1989 and infected dozens of monkeys in separate research rooms, highlighting the current potential of an airborne Ebola strain killing millions of people.
In late 1989, cynomolgus monkeys from the Philippines delivered to Hazleton Research Products’ Primate Quarantine Unit in Reston, Va., began dying at an alarming rate, prompting HRP to euthanize all the monkeys in that shipment, but during the 10 days after the euthanization, other monkeys in separate rooms connected only by air ducts began dying as well, which was attributed to an Ebola strain that went airborne.
“Due to the spread of infection to animals in all parts of the quarantine facility, it is likely that Ebola Reston may have been spread by airborne transmission,” wrote Lisa A. Beltz in the book Emerging Infectious Diseases. “On several subsequent occasions during 1989, 1990 and 1996, Ebola Reston killed monkeys in colonies in the United States.”
“Some of the people at the colony in Texas and several of the workers at the facility in the Philippines also produced antibodies to the virus but did not become ill.”
The 1989 incident validates concerns that a new, airborne strain of Ebola could infect humans, and if such a mutated strain already exists, it would easily explain why Ebola is currently spreading so rapidly in Africa.
For one thing, because Ebola doesn’t replicate itself perfectly every time it infects a victim, each new infection represents a potential mutation of the disease.
“If certain mutations occurred, it would mean that just breathing would put one at risk of contracting Ebola,” wrote Michael T. Osterholm of the New York Times. “Infections could spread quickly to every part of the globe, as the H1N1 influenza virus did in 2009, after its birth in Mexico.”
And due to the severity of the current outbreak in western Africa, which is the worst in history, Ebola has had more chances to mutate in the past four months than in the past 500 years.
“What is not getting said publicly, despite briefings and discussions in the inner circles of the world’s public health agencies, is that we are in totally uncharted waters and that Mother Nature is the only force in charge of the crisis at this time,” journalist Mac Slavo wrote.
What is known publicly, however, is that the State Department has taken the threat of Ebola so seriously it recently ordered 160,000 Hazmat suits, well over 100 times the number of federal workers currently in western Africa.
But just how large is the risk of Ebola mutating even further? Right now, it has the potential to infect – and kill – five million people in western Africa, according to a top German virologist.
“The right time to get this epidemic under control in these countries has been missed,” Jonas Schmidt-Chanasit of Hamburg’s Bernhard Nocht Institute for Tropical Medicine told Deutsche Welle. “That time was May and June; now it is too late.”
In late 1989, cynomolgus monkeys from the Philippines delivered to Hazleton Research Products’ Primate Quarantine Unit in Reston, Va., began dying at an alarming rate, prompting HRP to euthanize all the monkeys in that shipment, but during the 10 days after the euthanization, other monkeys in separate rooms connected only by air ducts began dying as well, which was attributed to an Ebola strain that went airborne.
“Due to the spread of infection to animals in all parts of the quarantine facility, it is likely that Ebola Reston may have been spread by airborne transmission,” wrote Lisa A. Beltz in the book Emerging Infectious Diseases. “On several subsequent occasions during 1989, 1990 and 1996, Ebola Reston killed monkeys in colonies in the United States.”
“Some of the people at the colony in Texas and several of the workers at the facility in the Philippines also produced antibodies to the virus but did not become ill.”
The 1989 incident validates concerns that a new, airborne strain of Ebola could infect humans, and if such a mutated strain already exists, it would easily explain why Ebola is currently spreading so rapidly in Africa.
For one thing, because Ebola doesn’t replicate itself perfectly every time it infects a victim, each new infection represents a potential mutation of the disease.
“If certain mutations occurred, it would mean that just breathing would put one at risk of contracting Ebola,” wrote Michael T. Osterholm of the New York Times. “Infections could spread quickly to every part of the globe, as the H1N1 influenza virus did in 2009, after its birth in Mexico.”
And due to the severity of the current outbreak in western Africa, which is the worst in history, Ebola has had more chances to mutate in the past four months than in the past 500 years.
“What is not getting said publicly, despite briefings and discussions in the inner circles of the world’s public health agencies, is that we are in totally uncharted waters and that Mother Nature is the only force in charge of the crisis at this time,” journalist Mac Slavo wrote.
What is known publicly, however, is that the State Department has taken the threat of Ebola so seriously it recently ordered 160,000 Hazmat suits, well over 100 times the number of federal workers currently in western Africa.
But just how large is the risk of Ebola mutating even further? Right now, it has the potential to infect – and kill – five million people in western Africa, according to a top German virologist.
“The right time to get this epidemic under control in these countries has been missed,” Jonas Schmidt-Chanasit of Hamburg’s Bernhard Nocht Institute for Tropical Medicine told Deutsche Welle. “That time was May and June; now it is too late.”
Image Credits: niaid, Flickr
WHAT IS NOT BEING SAID PUBLICLY:
EBOLA VIRUS’S HYPER-EVOLUTION IS UNPRECEDENTED… COULD GO AIRBORNE
According to officials, the concern is that it has had
an opportunity to mutate and it could eventually go airborne
EBOLA VIRUS’S HYPER-EVOLUTION IS UNPRECEDENTED… COULD GO AIRBORNE
According to officials, the concern is that it has had
an opportunity to mutate and it could eventually go airborne
by MAC SLAVO | SHTFPLAN.COM SEPTEMBER 14, 2014
The last several months have led to much confusion about the spread of the Ebola virus. Health officials and governments first denied that a serious threat existed and took no significant action to prevent its spread outside of West Africa. Then, after it had made it’s way to six different countries in the region, officials at the World Health Organization and the U.S. Centers for Disease Control started to panic. Apathy gave way to the real fear that we were facing a virus on a whole different scale than ever before.
At its current rate, some mathematical models show that the virus could infect anywhere from 20,000 to 100,000 by the end of the year, with over 4,000 people worldwide having been infected thus far. About 2,300 people, over 50% of those who have contracted it, have died.
Although the CDC released a recent report warning travelers that the virus could leave infectious material in the air, they were careful to say that it was not capable of spreading like other airborne viruses such as the common cold or flu.
But, with the way the virus has mutated and spread thus far, to say that the world’s top medical professionals and health officials are worried would be an understatement. Ebola has contacted more humans in the last 9 months than all previous outbreaks over the last 40 years combined. The concern, according to officials, is that it has had an opportunity to mutate and it could eventually go airborne.
What is not getting said publicly, despite briefings and discussions in the inner circles of the world’s public health agencies, is that we are in totally uncharted waters and that Mother Nature is the only force in charge of the crisis at this time.
There are two possible future chapters to this story that should keep us up at night.
The first possibility is that the Ebola virus spreads from West Africa to megacities in other regions of the developing world. This outbreak is very different from the 19 that have occurred in Africa over the past 40 years. It is much easier to control Ebola infections in isolated villages. But there has been a 300 percent increase in Africa’s population over the last four decades, much of it in large city slums. What happens when an infected person yet to become ill travels by plane to Lagos, Nairobi, Kinshasa or Mogadishu — or even Karachi, Jakarta, Mexico City or Dhaka?
The second possibility is one that virologists are loath to discuss openly but are definitely considering in private: that an Ebola virus could mutate to become transmissible through the air. You can now get Ebola only through direct contact with bodily fluids. But viruses like Ebola are notoriously sloppy in replicating, meaning the virus entering one person may be genetically different from the virus entering the next.
The current Ebola virus’s hyper-evolution is unprecedented; there has been more human-to-human transmission in the past four months than most likely occurred in the last 500 to 1,000 years. Each new infection represents trillions of throws of the genetic dice.
If certain mutations occurred, it would mean that just breathing would put one at risk of contracting Ebola.
Source: New York Times
In the event of the Ebola virus going airborne, research models show that it would quickly spread to all corners of the globe, infecting and killing millions.
At its current rate, some mathematical models show that the virus could infect anywhere from 20,000 to 100,000 by the end of the year, with over 4,000 people worldwide having been infected thus far. About 2,300 people, over 50% of those who have contracted it, have died.
Although the CDC released a recent report warning travelers that the virus could leave infectious material in the air, they were careful to say that it was not capable of spreading like other airborne viruses such as the common cold or flu.
But, with the way the virus has mutated and spread thus far, to say that the world’s top medical professionals and health officials are worried would be an understatement. Ebola has contacted more humans in the last 9 months than all previous outbreaks over the last 40 years combined. The concern, according to officials, is that it has had an opportunity to mutate and it could eventually go airborne.
What is not getting said publicly, despite briefings and discussions in the inner circles of the world’s public health agencies, is that we are in totally uncharted waters and that Mother Nature is the only force in charge of the crisis at this time.
There are two possible future chapters to this story that should keep us up at night.
The first possibility is that the Ebola virus spreads from West Africa to megacities in other regions of the developing world. This outbreak is very different from the 19 that have occurred in Africa over the past 40 years. It is much easier to control Ebola infections in isolated villages. But there has been a 300 percent increase in Africa’s population over the last four decades, much of it in large city slums. What happens when an infected person yet to become ill travels by plane to Lagos, Nairobi, Kinshasa or Mogadishu — or even Karachi, Jakarta, Mexico City or Dhaka?
The second possibility is one that virologists are loath to discuss openly but are definitely considering in private: that an Ebola virus could mutate to become transmissible through the air. You can now get Ebola only through direct contact with bodily fluids. But viruses like Ebola are notoriously sloppy in replicating, meaning the virus entering one person may be genetically different from the virus entering the next.
The current Ebola virus’s hyper-evolution is unprecedented; there has been more human-to-human transmission in the past four months than most likely occurred in the last 500 to 1,000 years. Each new infection represents trillions of throws of the genetic dice.
If certain mutations occurred, it would mean that just breathing would put one at risk of contracting Ebola.
Source: New York Times
In the event of the Ebola virus going airborne, research models show that it would quickly spread to all corners of the globe, infecting and killing millions.
U.S. hospitals are already preparing intake areas in case the virus hits home and a Congressional report released earlier this year says that Ebola detection kits and mobile response facilities have been deployed to National Guard units in all fifty states.
Thus, while the public remains oblivious to the seriousness of the threat, the government is rapidly ramping up preparations.
However, it may all be for naught should the current Ebola strains become transmissable by air. In such an event millions will contract the virus and the medical systems in the United States will be overwhelmed. Moreover, any experimental vaccines may be slow in coming due to massive global demand and limited supplies.
This leaves prevention on an individual scale the only viable strategy. Tess Pennington, author of The Prepper’s Blueprint, recommends that every family prepare a sick room and stock up on some essential pandemic preparedness supplies (not just for Ebola but any potential contagion outbreak in the future).
The very basic considerations in such a scenario should include methods of quarantining those suspected of having contracted an illness and protective equipment for those providing treatment. This might include WHO recommended N-100 respirator masks, Tyvek body suits, protective eyewear, gloves and shoe coverings.
Moreover, should such an event grip the world, millions of people would be in panic mode. Normal systems of commerce would likely break down, leaving many without food, clean water, and power. Thus, preparing for a scenario where the world as we know it literally comes to a screeching halt is also important to consider.
To be clear, Ebola has not yet achieved an airborne mutation in humans that we are aware of (though research has shown that it has been carried by breathing between animals). But, just because it has happened yet, doesn’t mean it can’t, especially considering the number of official cases reported so far.
In 1918 the Spanish flu killed as many as 50 million people, roughly 5% of the world’s population. Can you imagine the implications of an airborne Ebola virus with a mortality rate of 50% to 90%?
Thus, while the public remains oblivious to the seriousness of the threat, the government is rapidly ramping up preparations.
However, it may all be for naught should the current Ebola strains become transmissable by air. In such an event millions will contract the virus and the medical systems in the United States will be overwhelmed. Moreover, any experimental vaccines may be slow in coming due to massive global demand and limited supplies.
This leaves prevention on an individual scale the only viable strategy. Tess Pennington, author of The Prepper’s Blueprint, recommends that every family prepare a sick room and stock up on some essential pandemic preparedness supplies (not just for Ebola but any potential contagion outbreak in the future).
The very basic considerations in such a scenario should include methods of quarantining those suspected of having contracted an illness and protective equipment for those providing treatment. This might include WHO recommended N-100 respirator masks, Tyvek body suits, protective eyewear, gloves and shoe coverings.
Moreover, should such an event grip the world, millions of people would be in panic mode. Normal systems of commerce would likely break down, leaving many without food, clean water, and power. Thus, preparing for a scenario where the world as we know it literally comes to a screeching halt is also important to consider.
To be clear, Ebola has not yet achieved an airborne mutation in humans that we are aware of (though research has shown that it has been carried by breathing between animals). But, just because it has happened yet, doesn’t mean it can’t, especially considering the number of official cases reported so far.
In 1918 the Spanish flu killed as many as 50 million people, roughly 5% of the world’s population. Can you imagine the implications of an airborne Ebola virus with a mortality rate of 50% to 90%?

Image Credits: European Commission / Flickr
VIROLOGIST: ‘IT’S TOO LATE,
EBOLA WILL KILL 5 MILLION’
Expert says virus will infect entire population of African countries
EBOLA WILL KILL 5 MILLION’
Expert says virus will infect entire population of African countries
by PAUL JOSEPH WATSON SEPTEMBER 12, 2014
A top German virologist has caused shockwaves by asserting that it’s too late to halt the spread of Ebola in Sierra Leone and Liberia and that five million people will die, noting that efforts should now be focused on stopping the transmission of the virus to other countries.
Jonas Schmidt-Chanasit of the Bernhard Nocht Institute for Tropical Medicine in Hamburg told Germany’s Deutsche Welle that hope is all but lost for the inhabitants of Sierra Leone and Liberia and that the virus will only “burn itself out” when it has infected the entire population and killed five million people.
“The right time to get this epidemic under control in these countries has been missed,” said Schmidt-Chanasit. “That time was May and June. “Now it is too late.”
The current Ebola outbreak in West Africa has killed over 2200 people, with Liberia and Sierra Leone accounting for over 1700 of those fatalities.
While calling for “massive help” from the international community to prevent Ebola appearing in other countries like Nigeria and Senegal, Schmidt-Chanasit warns that getting a grip on the epidemic in Liberia and Sierra Leone is a departure from reality.
German aid organization Welthungerhilfe blasted Schmidt-Chanasit for his comments, with Sierra Leone based coordinator Jochen Moninger labeling his statements, “dangerous and moreover, not correct.” However, Moninger acknowledged that Schmidt-Chanasit’s assessment may be accurate in the case of Liberia.
The World Health Organization refused to comment on Schmidt-Chanasit’s remarks.
Although Ebola continues to rage in five African countries, media coverage of the epidemic has waned, despite evidence that the virus has mutated.
As we reported last month, former FDA official Scott Gottlieb, M.D. warned that if the virus was to hit the United States, the CDC would enact emergency procedures which could lead to healthy Americans who show no symptoms of the diseased being forcibly detained for an indefinite period of time.
Scientists in Canada and Canada’s Public Health Agency have both acknowledged that the virus has likely gone airborne at least to a limited degree, while the CDC has urged airline staff to take steps to prevent the airborne spread of the virus, including giving suspected Ebola victims surgical masks as well as directing staff to “not use compressed air, which might spread infectious material through the air.”
UPDATE: After this article was published, the “5 million” quote from the original Deutsche Welle report was removed and the headline was changed. The original text can be read here. It is not known why Deutsche Welle changed the wording of the report without issuing a formal retraction.
After my report, Deutsche Welle changed their headline and removed the '5 million dead' quote from their article. pic.twitter.com/hPFpByxKPb
— Paul Joseph Watson (@PrisonPlanet) September 12, 2014
Facebook @ https://www.facebook.com/paul.j.watson.71
FOLLOW Paul Joseph Watson @ https://twitter.com/PrisonPlanet
Jonas Schmidt-Chanasit of the Bernhard Nocht Institute for Tropical Medicine in Hamburg told Germany’s Deutsche Welle that hope is all but lost for the inhabitants of Sierra Leone and Liberia and that the virus will only “burn itself out” when it has infected the entire population and killed five million people.
“The right time to get this epidemic under control in these countries has been missed,” said Schmidt-Chanasit. “That time was May and June. “Now it is too late.”
The current Ebola outbreak in West Africa has killed over 2200 people, with Liberia and Sierra Leone accounting for over 1700 of those fatalities.
While calling for “massive help” from the international community to prevent Ebola appearing in other countries like Nigeria and Senegal, Schmidt-Chanasit warns that getting a grip on the epidemic in Liberia and Sierra Leone is a departure from reality.
German aid organization Welthungerhilfe blasted Schmidt-Chanasit for his comments, with Sierra Leone based coordinator Jochen Moninger labeling his statements, “dangerous and moreover, not correct.” However, Moninger acknowledged that Schmidt-Chanasit’s assessment may be accurate in the case of Liberia.
The World Health Organization refused to comment on Schmidt-Chanasit’s remarks.
Although Ebola continues to rage in five African countries, media coverage of the epidemic has waned, despite evidence that the virus has mutated.
As we reported last month, former FDA official Scott Gottlieb, M.D. warned that if the virus was to hit the United States, the CDC would enact emergency procedures which could lead to healthy Americans who show no symptoms of the diseased being forcibly detained for an indefinite period of time.
Scientists in Canada and Canada’s Public Health Agency have both acknowledged that the virus has likely gone airborne at least to a limited degree, while the CDC has urged airline staff to take steps to prevent the airborne spread of the virus, including giving suspected Ebola victims surgical masks as well as directing staff to “not use compressed air, which might spread infectious material through the air.”
UPDATE: After this article was published, the “5 million” quote from the original Deutsche Welle report was removed and the headline was changed. The original text can be read here. It is not known why Deutsche Welle changed the wording of the report without issuing a formal retraction.
After my report, Deutsche Welle changed their headline and removed the '5 million dead' quote from their article. pic.twitter.com/hPFpByxKPb
— Paul Joseph Watson (@PrisonPlanet) September 12, 2014
Facebook @ https://www.facebook.com/paul.j.watson.71
FOLLOW Paul Joseph Watson @ https://twitter.com/PrisonPlanet

Image Credits: Wikimedia Commons
CDC CONCERNED ABOUT AIRBORNE
TRANSMISSION OF EBOLA VIRUS
Federal agency directs airline staff to prevent spread of
"infectious material through the air"
by PAUL JOSEPH WATSON AUGUST 4, 2014
Despite repeated assurances that the Ebola virus cannot be transmitted via airborne particles, the CDC is concerned about that very outcome and has directed airline staff to take steps to prevent the spread of “infectious material through the air.”
While Ebola is highly contagious, the risk of a full blown pandemic has been downplayed by health authorities because, according to our current understanding of the virus, Ebola, “is not airborne and is transmitted through contact with bodily fluids, including sweat and blood.”
However, with concerns rising that the current strain of the virus, which is the worst in history and has killed 887 people, could in fact be airborne, the Centers For Disease Control has implemented steps to prevent its spread via international air travel.
A CDC advisory entitled Interim Guidance about Ebola Virus Infection for Airline Flight Crews, Cleaning Personnel, and Cargo Personnel reveals that the federal agency is concerned about airborne contamination.
The advisory urges airline staff to provide surgical masks to potential Ebola victims in order “to reduce the number of droplets expelled into the air by talking, sneezing, or coughing.” (emphasis mine).
The CDC is also directing airline cleaning personnel to, “not use compressed air, which might spread infectious material through the air.” (emphasis mine).
The CDC’s concern about the Ebola virus being spread via the air is understandable in light of a 2012 experiment conducted by Canadian scientists which proved that, “the ebola virus could be transmitted by air between species.”
Researchers demonstrated that the virus could be transmitted from pigs to monkeys without any direct contact by placing the two animals in pens separated only by a wire barrier. After eight days, some of the monkeys were found to have symptoms of Ebola likely as a result of “inhaling large aerosol droplets produced from the respiratory tracts of the pigs.”
The results of the study led scientists to conclude that, “limited airborne transmission might be contributing to the spread of the disease in some parts of Africa,” although they cautioned against making comparisons to the airborne nature of the influenza virus.
In addition, the Public Health Agency of Canada’s official website states under a section entitled “mode of transmission,” that “airborne spread among humans is strongly suspected, although it has not yet been conclusively demonstrated.”
The potential for a new strain of the Ebola virus to have achieved airborne transmission only serves to cast further doubt on the logic of the United States choosing to import two Ebola sufferers into the country.
As we reported last week, President Barack Obama signed an amendment to executive order which allows health authorities to detain Americans who merely show signs of respiratory illness.
The CDC has also outlined measures for dealing with an outbreak of a communicable disease which allow for the quarantine of “well persons” who “do not show symptoms” of the disease.
Facebook @ https://www.facebook.com/paul.j.watson.71
FOLLOW Paul Joseph Watson @ https://twitter.com/PrisonPlanet
Despite repeated assurances that the Ebola virus cannot be transmitted via airborne particles, the CDC is concerned about that very outcome and has directed airline staff to take steps to prevent the spread of “infectious material through the air.”
While Ebola is highly contagious, the risk of a full blown pandemic has been downplayed by health authorities because, according to our current understanding of the virus, Ebola, “is not airborne and is transmitted through contact with bodily fluids, including sweat and blood.”
However, with concerns rising that the current strain of the virus, which is the worst in history and has killed 887 people, could in fact be airborne, the Centers For Disease Control has implemented steps to prevent its spread via international air travel.
A CDC advisory entitled Interim Guidance about Ebola Virus Infection for Airline Flight Crews, Cleaning Personnel, and Cargo Personnel reveals that the federal agency is concerned about airborne contamination.
The advisory urges airline staff to provide surgical masks to potential Ebola victims in order “to reduce the number of droplets expelled into the air by talking, sneezing, or coughing.” (emphasis mine).
The CDC is also directing airline cleaning personnel to, “not use compressed air, which might spread infectious material through the air.” (emphasis mine).
The CDC’s concern about the Ebola virus being spread via the air is understandable in light of a 2012 experiment conducted by Canadian scientists which proved that, “the ebola virus could be transmitted by air between species.”
Researchers demonstrated that the virus could be transmitted from pigs to monkeys without any direct contact by placing the two animals in pens separated only by a wire barrier. After eight days, some of the monkeys were found to have symptoms of Ebola likely as a result of “inhaling large aerosol droplets produced from the respiratory tracts of the pigs.”
The results of the study led scientists to conclude that, “limited airborne transmission might be contributing to the spread of the disease in some parts of Africa,” although they cautioned against making comparisons to the airborne nature of the influenza virus.
In addition, the Public Health Agency of Canada’s official website states under a section entitled “mode of transmission,” that “airborne spread among humans is strongly suspected, although it has not yet been conclusively demonstrated.”
The potential for a new strain of the Ebola virus to have achieved airborne transmission only serves to cast further doubt on the logic of the United States choosing to import two Ebola sufferers into the country.
As we reported last week, President Barack Obama signed an amendment to executive order which allows health authorities to detain Americans who merely show signs of respiratory illness.
The CDC has also outlined measures for dealing with an outbreak of a communicable disease which allow for the quarantine of “well persons” who “do not show symptoms” of the disease.
Facebook @ https://www.facebook.com/paul.j.watson.71
FOLLOW Paul Joseph Watson @ https://twitter.com/PrisonPlanet
BioAcoustic Biology Research Studio investigates public information and research to incorporate every aspect of everything that affects public health and emotional peace of mind. We are a Research/Education site. Finding TRUE KNOWLEDGE is very hard these days. We are committed to supplying you with all that we can find on a given subject, it is then up to you, to use YOUR DISCERNMENT, to truly know the reality we all share. This is a research, education and self help site. We are all in this together, the more EVERYONE KNOWS, the better off we ALL will be.
Disclaimer: the posting of stories, commentaries, reports, research, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein. This site is not affiliated with any government, religious, philosophical or political organizations.
Disclaimer: the posting of stories, commentaries, reports, research, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein. This site is not affiliated with any government, religious, philosophical or political organizations.
